
Pharmacogenetic testing for biologic medications? Myth vs reality
Updated June 2022
The escalating cost of biologic medications has private and public plan sponsors concerned. As a result, many are turning to new technologies to stratify patient populations with the aim of reducing the total cost of biologics. For example, some providers are looking to pharmacogenetic (PGx) tests to guide drug therapy selection, including biologics. Others are looking at substituting branded biologics with biosimilars. A biosimilar, or “generic biologic,” is a biopharmaceutical drug designed to have active properties similar to a branded biological medicine. In reality, most genetic tests currently lack the specificity, sensitivity, and clinical validation to be helpful for this purpose. Unlike PGx tests, like Pillcheck, that effectively predict response for non-biologics, similar predictive testing for non-cancer biologics for other chronic conditions is in an earlier stage of development and not yet validated.
Genomics-guided cancer therapy
Since biological medications treat complex conditions, such as autoimmune diseases and cancer, a careful selection of candidate patients can improve efficacy and cost-efficiency. For example, in oncology, biologics are designed to block the activity of specific gene mutations which drive cancer growth. For this reason, a companion test at the time of tumor biopsy (performed by special pathology laboratories) is used to determine candidates for biological medications. Genomics-guided cancer therapy has become standard of care because this approach greatly improved patient response and reduced treatment toxicity.
Complex nature of autoimmune diseases hinders genomic targeting
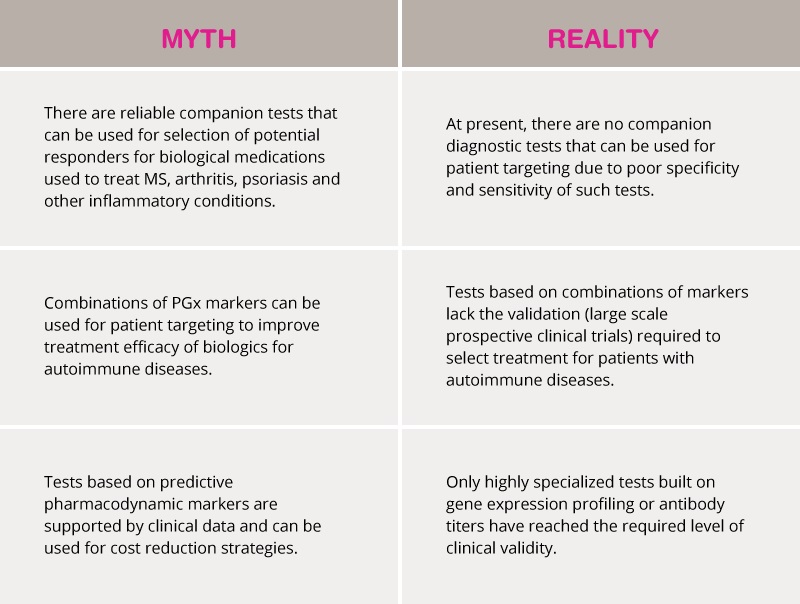
Autoimmune conditions are triggered by a complex interaction of hundreds of different genetic and environmental factors. Therefore, it is exceptionally hard to find reliable markers that predict response to biologics such as TNF inhibitors, IL-6 blockers and other drugs targeting the immune system. At present, there are no companion diagnostic tests that could be used for patient targeting – i.e. selection of potential responders – for biological medications for MS, arthritis, psoriasis and other inflammatory conditions.
Although the PharmGKB database has references to hundreds of genetic markers associated with biologics, these markers, or even multiplexed combinations of PGx markers, cannot be used to target patients due to the poor specificity and sensitivity of such tests. In addition, pharmacogenetic tests that combine pharmacodynamic markers still require validation in large-scale prospective clinical trials to assess whether such tests can improve treatment efficacy for autoimmune diseases. The use of non-validated PGx tests to select treatment can pose risks for patients with autoimmune disease as treatment failure can lead to disability. In contrast, PGx tests for non-biologic medications are more robust because they are built on direct correlations of drug concentration in the blood and pharmacokinetic gene variations. Using such tests for non-biologic medicine has been shown to improve the safety of treatment.
Specialized tests predicting clinical response to biologics
Many biologics are monoclonal antibodies for treating cancer and autoimmune conditions, such as multiple sclerosis (MS), rheumatoid arthritis (RA), and Irritable Bowel Disease (IBD). At present, only highly specialized tests of blood samples are used to monitor drug levels and clinical response. For example, the Vectra DA test is an RA disease activity test offered by Myriad Genetics to help physicians assess response to treatment and the risk of joint damage. Vectra DA can potentially guide second-line treatment after methotrexate and inform biologic tapering decisions for patients in stable remission. Such a test would be applicable for both branded biologics and biosimilars.
Antibody titer tests are currently available for therapeutic monitoring of infused monoclonal antibody levels, which are the active form of a biologic medication. These tests have been developed primarily to test how frequently the patient should be re-infused. However, such tests may be specific to a branded drug manufacturer and may need re-validation for biosimilars.
Cancer-related testing |
Rheumatoid arthritis, IBD, MS testing |
| Assesses if biomarker is present in the tumour | Multiple immune response genes |
| Presence of a single mutation can be a strong predictor of treatment response or resistance | Even multiple variants cannot predict response |
| Genomics is standard of care to guide therapy options | Genomics cannot yet guide therapy |
| Response to treatment monitored by imaging and circulating tumour DNA (ctDNA) | Drug (antibody) titer is a good predictor of response. |
Summary
- Valid cost reduction strategies should include generic substitution for branded biologics and antibody tiger testing.
- Other types of pharmacogenomic testing to predict response to biologics for autoimmune diseases are still in the early stages of clinical development and validation.
- Pharmacogenetic tests, such as Pillcheck, can assess the suitability of non-biologic alternative treatments.
- PGx testing for non-biologic drugs, which constitute the largest volume of drug claims, has been clinically proven and can reduce disability claims and eliminate waste on ineffective drugs.
References
Conti V et al., Biomarkers to Personalize the Treatment of Rheumatoid Arthritis: Focus on Autoantibodies and Pharmacogenetics. Biomolecules. 2020 Dec 14;10(12):1672.
Ditto MC et al., Efficacy and safety of a single switch from etanercept originator to etanercept biosimilar in a cohort of inflammatory arthritis. Sci Rep. 2020 Sep 30;10(1):16178.
Eser A et al., Increased Induction Infliximab Clearance Predicts Early Antidrug Antibody Detection. .J Clin Pharmacol. 2021 Feb;61(2):224-233.
Pallio G et al., Polymorphisms Involved in Response to Biological Agents Used in Rheumatoid Arthritis. Biomolecules. 2020 Aug 19;10(9):1203.
